





This article is part of a series of articles on the topic of People-Centered Care originally published on LinkedIn as part of Beryl Institute’s Patient Experience Week 2022.
You can find the original LinkedIn article here.
—
Note: In this post, for the sake of brevity, the term “patients” can include any person involved with the health system for care or service, including those we would otherwise call residents, clients, etc. I may also use the broader term of “people with lived experience”. The acronym PCC will be used in place of People-Centred Care.
I’d also like to start today’s post with a caveat about the current state in healthcare related to the pandemic and its impacts on healthcare workers. The content in this post is intended to share the importance of partnering with staff and clinicians in creating improvements and change in healthcare. Right now, people are burned out and unwell and thinking about making change or engaging in quality improvement feels more daunting than ever before. We do know that the pandemic has highlighted even more aspects of our system that need to change, and our healthcare workforce hold so much key information and perspectives to help us identify those needed improvements and help us make them. I hope this post will help leaders and others to see that we all need to work together effectively and bring together all of the passion and innovative ideas that are held by our workforce busting their butts every day for all of us.
People-centred care is about all of the people who are involved in the healthcare system; the patients, the family members, the caregivers, the patient partners, the volunteers; but also the people involved in care delivery: staff, clinicians, and leaders.
The healthcare workforce is critical to high quality, safe, effective, and efficient PCC. Every organization must invest heavily in its workforce to achieve its goals. No matter how much an organization and its formal leaders believe in their vision, mission, and values (including PCC), if its workforce is not engaged, the organization will not achieve its objectives. It’s impossible to change culture, strategy, and processes successfully with a disengaged group of people.
Staff and clinician engagement is both an enabler and an outcome of PCC which has a profound impact on staff and clinician experience, and by extension, patient and family experience.
| Enabler- Engaging the team | Outcome – Staff feel engaged |
| Actively bringing staff and clinicians to the table to be involved in care design, delivery, and improvement so that we benefit from the valuable insights and expertise they bring to the table. | Staff who feel engaged are more likely to be present (physically and mentally), feel committed and passionate, take initiative, and innovate.
Staff who feel engaged are, in turn, able to better partner with patients and families to deliver the best possible care and experience every day. |
(CHA Learning, 2019)
What is staff and clinician engagement?
Engagement, in the context of staff and clinicians, is both about fostering relationships with the people you work with and valuing their roles, perspectives and ideas. This engagement may look different for each group or individual. It means connecting with them, knowing them, knowing how they feel about their work, what they are proud of in their work, and what keeps them up at night.
Engagement in this context also includes involving staff and clinicians in identifying issues, concerns, or opportunities for improvement and in decision-making processes: from vision and values development to strategic planning to policy development and implementation to quality and safety initiatives to co-designing programs, services, and spaces.
Why is staff and clinician engagement important?
Engaging patients and families is critical when designing, championing, and fostering PCC. Just as critical is engaging staff and clinicians. Without engaged staff and clinicians, you are missing key partners. If you do not involve the people who will be using or putting into practice the things you are designing, there will be flaws in the design. Or, even if the design is sound, people might not feel invested in and committed to the change. And, if staff are disengaged, they will be unable to effectively partner with patients and families. Whatever the change, people are more likely to support, own, and commit to what they help create – especially if it involves changing their behaviours.
When the right conditions for engagement exist, all members of an organization should feel supported to do their best work; they truly care about and can contribute to a shared organizational vision and objectives. Staff and clinicians are engaged when they feel valued, are emotionally connected, involved, enthusiastic, and committed to providing great care and service. When staff is engaged, they know what they do and say matters. They make a difference.
Engagement is not just about staff and clinician satisfaction. Research shows that staff and clinician engagement impacts the quality of care and safety. For example, the King’s Fund in the United Kingdom conducted research which showed that increases in employee engagement led to decreases in healthcare-acquired infections and overall mortality rates (West & Dawson, 2012).
When staff is highly engaged, they are more likely to follow safety protocols such as handwashing, not skipping steps, or important safety procedures. They are also better able to make effective clinical decisions and actions when they are present and well. Patient satisfactions scores also increased alongside staff engagement rates. Additionally, the study found that there are significant financial costs related to poor engagement because of absenteeism and stress-related illness.
The King’s Fund in the UK also specifies the following building blocks for harnessing the creativity and enthusiasm of staff (2015):
- Develop a compelling, shared strategic direction about staff and clinician engagement;
- Build collective and distributed leadership to give staff and clinicians ownership and leadership opportunities;
- Adopt supportive and inclusive leadership styles to create psychologically safe workplaces;
- Give staff the tools to lead service transformation to own and be responsible for change processes;
- Establish a culture based on integrity, trust, and shared values which support healthy relationships and positive work environment;
- Place staff engagement firmly on the board agenda to prioritize staff and clinician engagement and wellbeing from the top down with tangible action and resources.
How can we effectively engage staff and clinicians?
There are many techniques for engagement and one of the core principles is having staff at the table with patients and families in truly co-designing care, service, and improvements. But how do we inspire staff to be fully engaged and to be a part of creating a people-centred culture? One of the things we talk about in our People-Centred Care Program is unleashing intrinsic motivation.
Intrinsic motivation is “doing something for the inherent satisfaction that engaging in the activity provides” (Ryan & Deci, 2000). Intrinsic motivation is much more powerful and lasting than external sources of motivation (e.g., money, gifts, time off, praise), though the two can certainly complement one another. For many in healthcare, intrinsic motivation is what led them towards the field.
Tapping into sources of intrinsic motivation galvanizes people’s individual and collective commitment to act; in other words, “creating conditions for many people to carry forward a shared cause on the inherent value that one experiences in the activity” (IHI, 2018). Strong intrinsic motivation can also lead a person to stay the course even when external factors are negative. This can be positive (it means staff is committed to their roles) but can also be negative (it can lead to burnout and compassion fatigue, something we are unfortunately seeing a lot of at the moment).
Ways to unleash intrinsic motivation
Here are a few ways we can unleash intrinsic motivation and inspire staff and clinicians, and some also apply to patients and families:
Storytelling
Narratives or storytelling help to create shared values and inspiration for individuals, teams, and organizations. The IHI presents three elements of public narrative in the diagram below:
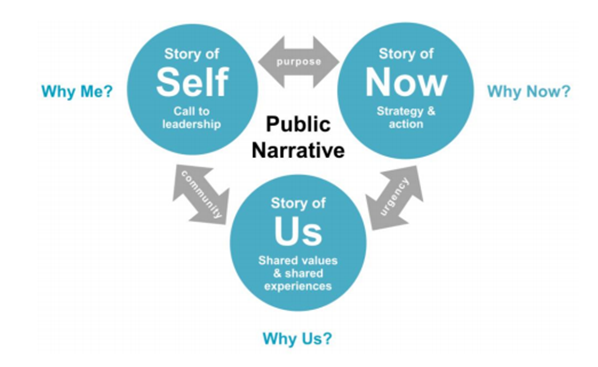
Three elements of public narrative. Reprinted from IHI Psychology of Change Framework to Advance and Sustain Improvement by Hilton K, Anderson. Copyright Institute for Healthcare Improvement 2018
- The story of self: Stories about our personal values that enable mindful action
- The story of us: Stories about values shared by a group of people engaged in action
- The story of now: Stories about the here and now that force us to respond mindfully, instead of reacting fearfully
Together, these three narrative elements support effective and proactive teamwork by addressing both opportunities and challenges. Organizations can use storytelling to build relationships amongst team members. Staff can share their stories in a safe space and learn about both personal and shared values and the challenges and opportunities ahead of them. Leaders may use this as part of teambuilding exercises or organizations could use this as a basis for developing training sessions that support culture development.
Motivational Task Design
Another way of unleashing intrinsic motivation is through designing tasks to promote intrinsic motivation in their execution. According to the IHI (2018), the conditions for motivational task design include:
- Meaningfulness: The task serves a purpose that is clear to me.
- Responsibility: I am responsible for how well the task is accomplished.
- Results: I know if I am doing a good job as I am doing it.
This creates a source of sustainable commitment and improvement as well as higher satisfaction and better work performance, lower absenteeism, and turnover (IHI, 2018).
A simple example of motivational task design is hand hygiene practice. Hand hygiene has been an area of focus for hospitals and healthcare organizations for many years, given the importance of this simple task in reducing the transmission of infection. Both staff and clinicians and patients and families have been engaged in hand hygiene initiatives, where:
- Staff, clinicians, patients, and families understand they need to accomplish this task in order to prevent the spread of infection.
- Responsibility. Each team member has the responsibility to wash their hands. Patients and families are encouraged to ask their providers if they have cleaned their hands before a healthcare encounter
- Results. Organizations routinely share data on infection rates, often by unit, so staff can see the impact they are having with good practices
Play and Celebrate
Staff should be encouraged to play and celebrate as part of improvement work; this builds additional motivation and psychologically reinforces the intrinsic motivation that already exists. Play is any recreational activity that occurs in a group or a team; it can be as involved as a teambuilding day engaging in a fun activity or as simple as playing short “icebreaker” games at the start of team meetings. Play allows staff to tap into creativity, imagination, relationship- and trust-building. It can occur at any point, and at any time.
Celebration, on the other hand, generally follows the conclusion of something; a change, a busy time period, etc. Celebration gives staff the opportunity to reflect on and honour contributions and successes and learn from failures (IHI, 2018). This builds and replenishes intrinsic motivation by rewarding people for a job well done.
Front-Line Ownership
The language “buy-in” has been used in describing a desired state in times of change or when an organization or leader is trying to introduce a new vision or way of doing things. This term really flies in the face of true engagement and investment in the change. In a people-centred organization, we don’t want our patients and families, staff and clinicians and other partners to simply agree with or accept our viewpoint. We want people to feel passionate, committed and part of the solution. We want partnership and ownership, not buy-in.
In 2013, Several Canadian healthcare researchers (Zimmerman et al) published a paper, Front-Line Ownership: Generating a Cure Mindset for Patient Safety. This paper was centred on a concept called front-line ownership (FLO) to support the advancement of patient safety and infection control practices. The concept of FLO can be applied to the advancement of PCC practice as well.
The researchers argued that healthcare workers need to be able to see a problem in order to take care of that problem, and that engagement of front-line staff is key to improvement. Traditionally, healthcare leaders try to “sell and promote ideas to front-line workers” to win buy-in (Zimmerman et al, 2013). FLO takes a different approach. FLO focuses on ownership: the concept that staff develop the ideas, make the decisions and design, and act on plans for change, instead of following practices that have been externally developed for them. FLO can be a powerful way to not only engage staff but also patients and families.
There are ten key principles associated with FLO:
- Accept rather than fight complexity, acknowledge local conditions.
- There is no right way to spread change
- Work with wiling participants
- Include the ”usual suspects” in your work
- Make the invisible visible
- Go slow to go fast, that is, give time for the group to determine the way forward
- Nothing about me, without me. That is, you cannot influence others if they are not invited.
- Act your way into a new way of thinking through gaining social proof.
- You want to achieve ownership, not buy-in.
- The path to improvement is rarely linear, but rather iterative and unpredictable.
(Gardam, Gitterman, Rykert, Vicencio & Baily, 2017)
In the People-Centred Care Program we also talk about the barriers to engagement as well as measuring staff and clinician engagement.
In summary, the engagement of and partnership with staff and clinicians is a critical component of people-centred care. It’s important to be clear that while there are separate activities and investments in engaging staff and clinicians, there are also many opportunities to partner with staff and clinicians AND patients and families together and those will be the most meaningful and impactful opportunities for change.
I’d also recommend one of CHA Learning’s recent podcast episodes featuring Jacqueline Per, Executive Director of Research and Innovation at Fraser Health in BC on the Future of Our Health Workforce, including the impacts of technology people who work within the health system. Check out the podcast here.
Tomorrow, I’ll shift gears and I’ll introduce you to a recent CHA Learning podcast with some real examples of patient partnership and support during the pandemic.
Today’s reflection/discussion question: What type of intrinsic motivator is the strongest for you personally in your work? Why do you think that is?